
Adderall vs. Vyvanse: A Clinician's Guide to Choosing the Right ADHD Medication for Your Child
Vyvanse and Adderall are both effective first-line stimulants for ADHD in children and teens — but they work very differently in the body, carry different abuse risk profiles, and fit different clinical situations. Dr. Marie Akers, DNP, PMHNP-BC, breaks down the key differences, explains what the research actually says, and helps parents understand which medication may be the right fit for their child.
Difference Between Vyvanse and Adderall for Kids
Every parent facing a new ADHD diagnosis for their child eventually arrives at the same question: Which medication is right? For the millions of children diagnosed with ADHD each year, stimulant medications remain the most effective pharmacologic treatment — and two of the most commonly prescribed are Adderall (mixed amphetamine salts) and Vyvanse (lisdexamfetamine). This guide breaks down the differences, explains when one may be preferred over the other, and highlights the tools available to help families and clinicians make this decision together.
---
Both Medications Work — and Work Well
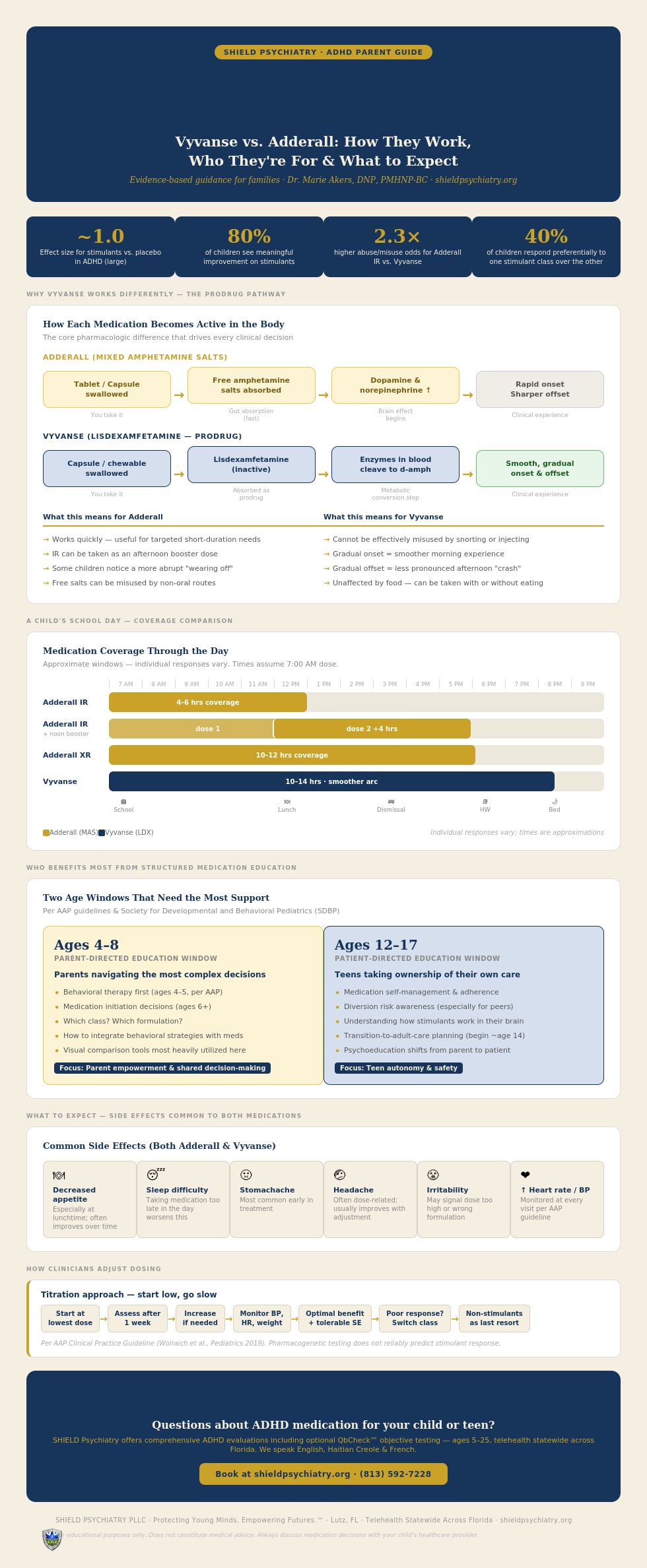
Adderall and Vyvanse belong to the same drug class: amphetamine-based stimulants. Large meta-analyses and the AAP Clinical Practice Guideline confirm that stimulants produce large effect sizes (~1.0) for ADHD symptom reduction in children and adolescents. A Cochrane review found no significant difference in efficacy between lisdexamfetamine, mixed amphetamine salts, and dexamphetamine. Roughly 40% of children respond well to both amphetamine and methylphenidate classes, while another 40% respond preferentially to one — meaning if the first choice doesn't work, the second very well might.
---
Which ADHD Medication is Better for Children: Vyvanse or Adderall?
So What's the Difference?
The core distinction is pharmacologic: Adderall delivers free amphetamine salts directly, while Vyvanse is a prodrug — it's inactive until the body's enzymes convert it to dextroamphetamine. This prodrug design has real clinical consequences:
- Smoother onset and offset: Vyvanse produces a more gradual pharmacokinetic arc, which can mean fewer "crash" symptoms at wear-off.
- Lower abuse potential: Because Vyvanse must be metabolized to become active, it cannot be effectively misused by crushing, snorting, or injecting. Poison center data show that abuse/misuse odds are 1.9–2.3× higher for Adderall formulations compared to Vyvanse.
- Longer duration: Vyvanse lasts 10–14 hours vs. 10–12 hours for Adderall XR and just 4–6 hours for Adderall IR.
On the other hand, Adderall offers advantages Vyvanse cannot:
- Dosing flexibility: The availability of both immediate-release (IR) and extended-release (XR) formulations allows clinicians to add an afternoon IR booster for homework time or use shorter coverage on weekends.
- Younger age approval: Adderall IR is FDA-approved for children as young as age 3, while Vyvanse is only approved for ages 6 and up.
- Lower cost: Generic mixed amphetamine salts are widely available and significantly less expensive. While generic lisdexamfetamine became available in 2023, supply variability persists.
---
When Might a Clinician Favor One Over the Other?
Consider Adderall when:
- The child is under age 6
- Flexible dosing is needed (e.g., short-acting booster for after-school activities)
- Cost is a primary concern
- A shorter coverage window is preferred
Consider Vyvanse when:
- Consistent all-day coverage is a priority (school through homework through evening activities)
- The child experiences harsh "crash" symptoms with other stimulants
- Abuse or diversion risk is a concern — particularly relevant for adolescents
- The child prefers a chewable tablet
- Appetite suppression or sleep disruption needs a smoother pharmacokinetic profile
---
Who Needs the Most Help Understanding These Choices?
Research and clinical guidelines highlight two groups that benefit most from visual aids and structured psychoeducation around ADHD treatment:
1. Parents of children ages 4–8 — This window encompasses the transition from behavioral-therapy-first (ages 4–5, per AAP) to medication initiation (ages 6+). Parents are navigating the most complex set of decisions: whether to medicate, which class, which formulation, and how to integrate behavioral strategies. Visual comparison tools, medication charts, and decision aids are most heavily utilized here.
2. Adolescents ages 12–17 — As teens take increasing ownership of their own care, psychoeducation shifts from parent-directed to patient-directed. Visual tools at this stage focus on medication self-management, adherence strategies, diversion risk awareness, and transition-to-adult-care planning (recommended to begin around age 14).
The Society for Developmental and Behavioral Pediatrics (SDBP) guideline emphasizes that psychoeducation must account for family literacy level, cultural context, and language to be effective — visual aids are not one-size-fits-all.
---
Parental Tools to Help Guide Shared Decision-Making
Tools for Shared Decision-Making
The AAP guideline makes a Grade A recommendation that family preference is essential in determining the treatment plan. Several resources can support this process:
- EBIADHD Platform (ebiadhd-database.org) — An open-access, continuously updated web tool developed alongside a 2025 BMJ umbrella review of 221 meta-analyses. It displays the effects and evidence certainty of every ADHD intervention across age groups and outcomes, designed specifically for shared decision-making.
- ADHDMedicationGuide.com — Referenced in the AAP guideline; lists all FDA-approved ADHD medications with key characteristics.
- CADDRA (Canadian ADHD Resource Alliance) — Provides free medication comparison charts, rating scales, and monitoring tools for primary care.
No single validated "Ottawa-style" decision aid has been widely adopted specifically for stimulant selection — the choice remains empirical and preference-driven. Pharmacogenetic testing does not reliably predict stimulant response.
---
What to Expect When A Child Starts Vyvanse or Adderall for ADHD?
- Improvement is often noticeable within the first week
- Clinicians start at a low dose and titrate upward weekly until the best balance of benefit and side effects is achieved
- Common side effects for both: decreased appetite, difficulty sleeping, stomachache, headache, irritability
- Blood pressure, heart rate, height, and weight should be monitored at every visit
- If one medication doesn't work well, switching within the amphetamine class or to the methylphenidate class is appropriate before considering nonstimulants
---
The Bottom Line
There is no universally "better" stimulant. Adderall and Vyvanse are both highly effective, and the right choice depends on the child's age, daily schedule, side-effect sensitivity, abuse risk profile, and family preferences. The most important step is not which medication is chosen first — it's the ongoing partnership between families and clinicians to monitor, adjust, and optimize treatment over time.
Ready to Find the Right Fit for Your Child?
If your child has been diagnosed with ADHD — or if you are wondering whether ADHD might be at the root of what you are seeing — I would love to help.
SHIELD Psychiatry offers comprehensive ADHD evaluations, including optional QbCheck™ objective ADHD testing, for children and teens ages 5 through 25. We see patients entirely via telehealth, statewide across Florida — including families in Tampa, Lutz, Wesley Chapel, Cheval, Westchase, Odessa, and throughout the state in Windermere, Winter Park, Naples, Sarasota, Palm Beach, Boca Raton, and Coral Gables.
I speak English, Haitian Creole, and French.
📞 (813) 592-7228 🌐 shieldpsychiatry.org
Book Now!! Your Child's ADHD Evaluation — Link: https://intakeq.com/new/rtc1xz
This post is for educational purposes only and does not constitute medical advice. Always discuss medication decisions with your child's licensed healthcare provider. SHIELD Psychiatry PLLC, 25200 Sawyer Francis Lane STE 135, Lutz, FL 33559.
REFERENCES:
Pediatrics. 2019. Wolraich ML, Hagan JF, Allan C, et al.Guideline
2.Comparison of Lisdexamfetamine and Dextroamphetamine Exposures Reported to U.S. Poison Centers.
Clinical Toxicology. 2015. Kaland ME, Klein-Schwartz W.Observational
3.LISDEXAMFETAMINE DIMESYLATE. FDA Drug Label. Food and Drug Administration. Updated date: 2026-05-07.